Drug-induced oral pigmentation can be caused by a variety of medications through multiple different mechanisms. Common culprit medications include minocycline, antimalarials, clofazimine, and oral contraceptives. Other implicated medications include zidovudine (azidothymidine; AZT), chlorpromazine, ketoconazole, busulfan, doxorubicin, bleomycin, cyclophosphamide, 5-fluorouracil, nicotine, heroin, nitrogen mustard, phenothiazines, arsenic, silver, gold, lead, mercury, progesterone, and imatinib mesylate.
The pathogenesis of oral pigment changes depends primarily on the causative drug. The drug or drug metabolites may be pigmented substances that can be identified lying free or chelated to iron or melanin within the hard and/or soft tissues. Minocycline complexes with iron and deposits in the mucosa. Hyperproduction of melanin through melanocyte stimulation has been implicated as the mechanism for antimalarial medications (chloroquine, hydroxychloroquine, amodiaquine, and quinacrine) as well as oral contraceptive pills. Amiodarone-induced oral pigmentation is thought to result from increased production of lipofuscin.
Other drugs may lead to oral pigmentation when a lichenoid drug eruption resolves with post-inflammatory hyperpigmentation (such as from nonsteroidal anti-inflammatory drugs or a number of antihypertensive medications) or when there is direct damage to the mucosa (such as from chemotherapeutic agents). An oral fixed drug eruption appears as one or more well-demarcated, round or oval, slate-brown colored macules. The most common offending agents are cotrimoxazole and tetracycline.
For a discussion addressing multiple possible etiologies of oral mucosal pigmentation (physiologic, exogenous and endogenous substances, systemic disease), see Multifocal or diffuse mucosal pigmentation.
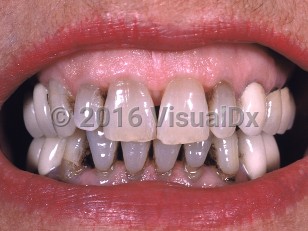
Drug-induced oral pigmentation - Oral Mucosal Lesion
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
T50.995A – Adverse effect of other drugs, medicaments and biological substances, initial encounter
SNOMEDCT:
403663003 – Drug-induced oral pigmentation
T50.995A – Adverse effect of other drugs, medicaments and biological substances, initial encounter
SNOMEDCT:
403663003 – Drug-induced oral pigmentation
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
Drug Reaction Data
Subscription Required
References
Subscription Required
Last Reviewed:05/24/2018
Last Updated:11/05/2019
Last Updated:11/05/2019
Drug-induced oral pigmentation - Oral Mucosal Lesion