Half-and-half nails, also known as Lindsay's nails, was first described in 1967 and is one of the most characteristic (but not pathognomonic) onychopathies seen in chronic renal failure. Although the exact pathogenesis is unclear, it is speculated that acidosis and an increase in toxic uremic substances occurring subsequent to sudden renal decompensation may stimulate melanin formation by nail matrix melanocytes.
Half-and-half nails are seen in an estimated 20%-50% of chronic renal failure patients. It is also seen in up to 84% of patients with azotemia and 8%-13% of hemodialysis patients; there is some debate whether the frequency of these changes correlates with duration of dialysis. Other reported causes include Kawasaki disease, hepatic cirrhosis, pellagra, zinc deficiency, chemotherapy, Behçet disease, and Crohn disease. Half-and-half nails have also been reported in patients without any systemic abnormality.
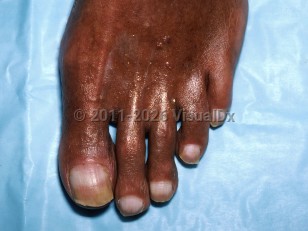
Fingernails are affected more often than toenails. Clinically, nails have a proximal pale pink or dull white "ground glass appearance" that is sharply demarcated from a red, pink, or brown distal portion. The transverse distal bands occupy 20%-60% of the total nail length.
There is no correlation between the distal band length and severity of renal failure. Furthermore, the half-and-half nail pattern is persistent, as there is no tendency of the bands to move with nail growth. Nonetheless, this phenomenon may reverse itself after successful renal transplantation, but not with hemodialysis or changes in hemoglobin or albumin levels.
Half and half nail syndrome - Nail and Distal Digit
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
L60.8 – Other nail disorders
SNOMEDCT:
50077007 – Half-and-half nail
L60.8 – Other nail disorders
SNOMEDCT:
50077007 – Half-and-half nail
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
Drug Reaction Data
Subscription Required
References
Subscription Required
Last Reviewed:06/24/2018
Last Updated:01/27/2025
Last Updated:01/27/2025
Half and half nail syndrome - Nail and Distal Digit