Generalized hypertrichosis:
- Congenital generalized hypertrichosis: Overgrowth of fine, gray to blond lanugo hairs at birth is consistent with congenital hypertrichosis lanuginosa, a rare condition in which lanugo hair is not replaced by normal vellus hairs. Lanugo hair grows to lengths up to 10 cm. There may be associated abnormalities of the eyes, ears, and gastrointestinal system. Babies born with overgrowth of pigmented, terminal hairs at birth should be evaluated for maternal drug or alcohol use and orofacial, skeletal, and/or neurologic abnormalities. Absence of these attributes and a family history of hypertrichosis support the diagnosis of benign familial hypertrichosis.
- Infantile generalized hypertrichosis: Drug-induced cases have been reported in infants whose caretakers were using minoxidil.
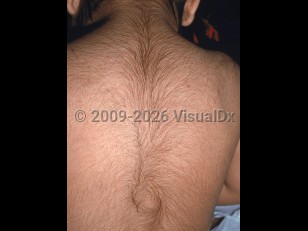
- Childhood generalized hypertrichosis: Progressive development of pigmented, terminal hairs during early childhood may occur in constitutional prepubertal hypertrichosis. However, disorders of androgen excess should be ruled out. A family history of hypertrichosis, Mediterranean or South Asian descent, "inverted fir tree" growth pattern on the back, and absence of other signs of early pubarche support the diagnosis of constitutional prepubertal hypertrichosis. Concurrent acne, axillary and pubic hair, and increased androgen levels raise suspicion for androgen excess.
- Adult generalized hypertrichosis: Acquired hypertrichosis lanuginosa is considered a paraneoplastic disorder, most often associated with lung, breast, and colon cancer. Patients should undergo malignancy screening. Overgrowth of pigmented, terminal hairs in adults may be related to underlying drug intake (most commonly minoxidil, phenytoin, and cyclosporine), hypothyroidism, malnutrition (including anorexia nervosa), traumatic brain injury, dermatomyositis, acrodynia, advanced HIV, or POEMS syndrome. A thorough review of systems should be obtained with relevant workup.
- Congenital and childhood localized hypertrichosis may be a localized developmental abnormality (eg, hairy elbow syndrome, hairy palms and soles, trichomegaly of the eyelashes, hypertrichosis of the auricle, hypertrichosis of the nasal tip, nevoid hypertrichosis), associated with an underlying hamartoma (eg, Becker nevus, congenital nevus, plexiform neurofibroma), or associated with an underlying genodermatosis (eg, porphyria cutanea tarda, Winchester syndrome, Rubinstein-Taybi syndrome, Cornelia de Lange syndrome, and many more). Hair growth focally over the spine should raise concern for spinal dyscrasia. A ring of hypertrichosis surrounding aplasia cutis (hair collar sign) may herald an underlying neurological defect.
- Adult acquired localized hypertrichosis may occur as a result of localized chronic inflammation or trauma, eg, at the site of a previous cast, sites of chronic rubbing due to chronic pruritus, and at sites of previous lupus panniculitis, morphea, or porphyrias (predominately porphyria cutanea tarda and variegate porphyria). Additionally, localized acquired hypertrichosis may be seen at sites of strong topical steroid application.