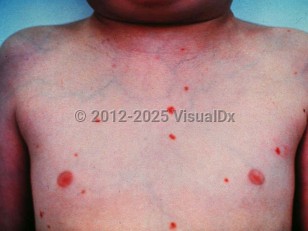
Sinus histiocytosis with massive lymphadenopathy, also known as Rosai-Dorfman disease and Rosai-Dorfman-Destombes disease, is a rare benign histiocytic proliferative disorder. Rosai-Dorfman disease usually appears in childhood and early adulthood (mean age of 20.6 years) and is somewhat more frequent in males (male predominance of 1.4:1). Classically, the patients present with prominent bilateral, massive, painless cervical lymphadenopathy, low-grade fever, weight loss, leukocytosis, elevated ESR, and polyclonal hypergammaglobulinemia. Extranodal involvement of at least one site is identified in 25%-43% of Rosai-Dorfman disease cases, and only 23% have exclusively extranodal disease. Skin is the most common site for extranodal involvement. Other documented sites of extranodal involvement include the respiratory tract, the skeletal system, the genital and urinary system, the central nervous system, the ocular system, the oral cavity, the salivary glands, breasts, and the cardiovascular system. Bone marrow is rarely involved. Cutaneous disease without involvement of lymph nodes or other organs is rare and is known as cutaneous Rosai-Dorfman disease.
Rarely, Rosai-Dorfman disease may be associated with other diseases including large B-cell lymphoma, myelodysplastic syndrome, plasmacytoma, idiopathic hypereosinophilic syndrome, Hodgkin lymphoma, sickle cell disease, and giant cell hepatitis. Other associated dermatologic conditions reported in the past include mycetoma, morphea, erythroderma, and Langerhans cell histiocytosis.
The etiology is not fully understood. It has been speculated that the initial histiocytic proliferation could be a result of an asymptomatic chronic infection or an abnormal exaggerated immune response to yet unknown antigen(s). Human herpesvirus 6 (HHV6) has been isolated from the involved tissue of some patients. Raised Epstein-Barr virus (EBV) and herpes simplex virus (HSV) antibody titers have also been reported. Associations with Klebsiella, Brucella, parvovirus B19, and cytomegalovirus have been suggested. Rosai-Dorfman disease has also been reported in HIV-infected individuals.
About one-third of patients with Rosai-Dorfman disease have mutually exclusive mutations in KRAS and MAP2K1.
Treatment is typically not necessary as the disease is self-limiting in most cases. Treatment is mainly needed to halt the natural progression only in a minority of patients where massive nodal or extranodal enlargement interferes with organ function or threatens life. The ideal treatment for Rosai-Dorfman disease should be tailored to the patient's individual situation.
Sinus histiocytosis with massive lymphadenopathy
Synopsis

Codes
ICD10CM:
D76.3 – Other histiocytosis syndromes
SNOMEDCT:
34287003 – Sinus histiocytosis with massive lymphadenopathy
D76.3 – Other histiocytosis syndromes
SNOMEDCT:
34287003 – Sinus histiocytosis with massive lymphadenopathy
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Updated:10/09/2024
Sinus histiocytosis with massive lymphadenopathy