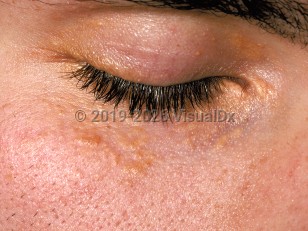
Xanthelasma palpebrarum (XP) is the most commonly encountered type of xanthoma and is classified as a type of localized plane xanthoma. It typically presents as yellowish macules or slightly elevated papules or plaques on the eyelids beginning in the fourth or fifth decade of life. XP involves the upper medial lids most prominently but may be more extensive, also involving the lower eyelids. The lesions are asymptomatic.
XP is approximately 3 times more common in women and does not appear to have any ethnic variation. Approximately half of patients with XP have a lipid disorder. While the majority of these cases occur in the setting of acquired hyperlipidemia, XP is also seen in the setting of type II hyperlipoproteinemia. XP has been shown to be an independent risk factor for atherosclerosis and, consequently, ischemic cardiovascular disease.
Xanthelasma palpebrarum - External and Internal Eye
Alerts and Notices
Important News & Links
Synopsis

Codes
ICD10CM:
H02.60 – Xanthelasma of unspecified eye, unspecified eyelid
SNOMEDCT:
238951005 – Xanthelasma
H02.60 – Xanthelasma of unspecified eye, unspecified eyelid
SNOMEDCT:
238951005 – Xanthelasma
Look For
Subscription Required
Diagnostic Pearls
Subscription Required
Differential Diagnosis & Pitfalls

To perform a comparison, select diagnoses from the classic differential
Subscription Required
Best Tests
Subscription Required
Management Pearls
Subscription Required
Therapy
Subscription Required
References
Subscription Required
Last Reviewed:05/17/2020
Last Updated:03/17/2022
Last Updated:03/17/2022
 Patient Information for Xanthelasma palpebrarum - External and Internal Eye
Patient Information for Xanthelasma palpebrarum - External and Internal Eye
Premium Feature
VisualDx Patient Handouts
Available in the Elite package
- Improve treatment compliance
- Reduce after-hours questions
- Increase patient engagement and satisfaction
- Written in clear, easy-to-understand language. No confusing jargon.
- Available in English and Spanish
- Print out or email directly to your patient
Upgrade Today

Xanthelasma palpebrarum - External and Internal Eye