Late or complicated presentations of acute cholecystitis can require care for sepsis, including intravenous (IV) line placement, antibiotic administration, and fluid resuscitation and/or pressor initiation, as appropriate.
Symptomatic management with analgesics and antiemetics should be provided, and surgical consultation should be initiated.
Diagnosis Overview:
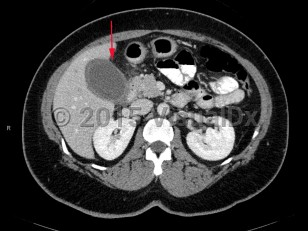
Acute cholecystitis is a surgical emergency of the biliary tract that can be life-threatening if appropriate treatment is not initiated promptly. Acute cholecystitis is characterized by gallbladder wall inflammation. Patients classically present with right upper quadrant (RUQ) abdominal pain, fever, and leukocytosis. Acute cholecystitis is further categorized by the presence of gallstones as calculous or acalculous.
Acute calculous cholecystitis: Constitutes 90%-95% of all cases. Gallstones obstruct the cystic duct, resulting in acute dilation and inflammation of the gallbladder wall. There are 2 primary types of gallstones:
- Cholesterol gallstones – Approximately 75% of all gallstones in the United States and Europe.
- Pigmented gallstones – Made of calcium bilirubinate and calcified bilirubin. This type of gallstone can be either black or brown. Black stones comprise approximately 20% of all gallstones and are found in patients with chronic hemolytic anemia, Gilbert syndrome, liver cirrhosis, or cystic fibrosis. Brown gallstones are more common in the Asian population, and they develop in the setting of chronic biliary tract infection such as parasitic infections.
Pathophysiology of acute cholecystitis: About 10%-15% of the general US population has gallstones, with the highest prevalence seen among individuals with American Indian ancestry and individuals with Hispanic ethnicity from Central and South America.
In most people, gallstones are asymptomatic. Biliary colic develops in 1%-4% of patients annually, and acute cholecystitis eventually develops in about 20% of patients with symptomatic gallstones if an elective cholecystectomy is not performed. The presence of gallstones alone is not predictive of acute cholecystitis. However, patients who are symptomatic from gallstones should consider cholecystectomy to prevent future development of acute cholecystitis.
Acute calculous cholecystitis occurs when a gallstone blocks the cystic duct, impairing gallbladder drainage. Temporary obstruction can cause biliary colic. Sustained obstruction can result in gallbladder dilation, wall inflammation, subsequent wall thickening, and pericholecystic fluid accumulation.
In early stages, gallbladder inflammation is sterile; however, secondary infection develops in most patients. Enteric organisms are most common, including Escherichia coli, Klebsiella, and Streptococcus faecalis.
Demographics and risk factors of acute cholecystitis:
Sex – Women are more likely to develop gallstones because of higher estrogen levels. For the same reason, pregnancy and hormone replacement therapy increase the risk of gallstones. Approximately 25% of women older than 60 years have gallstones. Cholecystitis develops in women more frequently due to the relative prevalence of gallstones.
Age – Gallstone incidence increases with age. Gallstones are unusual in children. In cases when they occur, they are commonly pigment stones. The following conditions put younger people and children at a higher risk of having gallstones:
- Spinal injury
- History of abdominal surgery
- Sickle cell disease
- Impaired immunity
- IV nutrition
Obesity and weight changes – In obesity, the liver overproduces cholesterol, which increases the risk of gallstone formation. Rapid weight loss is also a risk factor for the development of cholesterol gallstones. As such, gallstones are frequently observed after bariatric surgical procedures.
Pregnancy – Increase in cholesterol saturation of bile and impaired gallbladder contraction during pregnancy predispose to formation of cholesterol stones or biliary sludge.
Genetics – Having a family member with gallstones increases one's risk. Mutations of gene ABCG8 increase the risk of gallstone formation.
AIDS – Biliary disease occurs via 2 mechanisms in patients with AIDS:
- Acute acalculous cholecystitis
- AIDS cholangiopathy (commonly due to Cryptosporidium or cytomegalovirus)
Ascariasis – This is a geographical risk factor in regions of China and Southeast Asia. Ascariasis can cause cholecystitis, cholangitis, hepatic abscess, or pancreatitis.
Clinical manifestations of acute cholecystitis:
RUQ pain – Can be episodic or sustained, severe, and located in the RUQ or epigastrium that can radiate to the shoulder or back. Exacerbated by eating, particularly fatty meals, and at night. Pain from biliary colic is generally episodic, while acute cholecystitis is classically accompanied by prolonged episodes of pain.
Physical examination findings – Tenderness and guarding in the RUQ and Murphy's sign.
Murphy's sign –
- Arrest in inspiration while palpating the gallbladder during a deep breath.
- Sensitivity of 50%-60% and a high specificity of up to 79%-96%.
Related topic: chronic cholecystitis